
MP Biomedicals Urine Panel Test
Available formats
Test Cassette
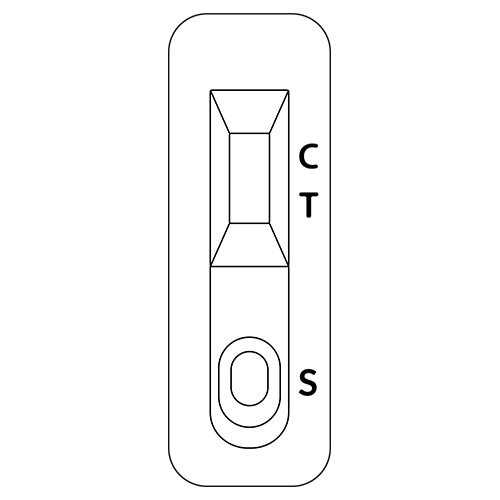
Single Drug Test
Test Cup

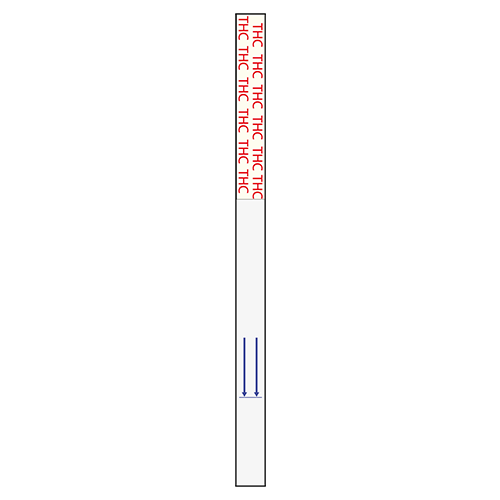
Test Dip Card
Test Cassette
Single Drug Test
Test Cup
Test Dip Card
Available Parameters
Ressources
Amphetamine (AMP)
Amphetamines are a class of potent sympathomimetic agents with therapeutic applications. The most common amphetamines are d-amphetamine and d, l-amphetamine. Amphetamines are central nervous stimulants that cause the neurotransmitters epinephrine, norepinephrine and dopamine to be released into the brain and body giving users feelings of euphoria, alertness, and increased energy. Chronic abuse of amphetamine leads to tolerance and drug reinforcement effect. Cardiovascular responses to amphetamine include increased blood pressure and cardiac arrhythmias. More acute responses produce anxiety, paranoia, hallucinations and psychotic behavior. Amphetamine is metabolized by several pathways. In general, acid urine promotes excretion whereas alkaline urine retards it. In 24 hours, approximately 79% of the amphetamine dose is excreted in acid urine and about 45% in alkaline urine. Typically, about 20% is excreted as unchanged amphetamine. Unchanged amphetamine can be detected up to 1 –2 days after use.
Benzodiazepine (BZD)
Benzodiazepines are a class of widely prescribed central nervous system depressants which have anxiolytic, hypnotic, anticonvulsant and muscle relaxant effects. Chronic abuse can result in addiction and tardive dyskinesia. Acute higher doses lead to drowsiness, dizziness, muscle relaxation, lethargy, coma and possible death. The effects of benzodiazepines use last 4 – 8 hours. Many of the benzodiazepines share a common metabolic route and are excreted as oxazepam and its glucuronide in urine. Oxazepam is detectable in the urine for up to 7 days after drug use.
Barbiturate (BAR)
Barbiturates are a group of prescription drugs that are frequently abused. They can depress the central nervous system. Acute higher dose induces exhilaration, sedation and respiratory depression. More acute responses produce respiratory collapse and coma. The effects of short-acting barbiturates, such as secobarbital last 3 to 6 hours. The effects of long-acting barbiturates such as phenobarbital last 10 to 20 hours. Short-acting barbiturates normally remain detectable in urine for 4 to 6 days, while long-acting barbiturates can be detected for up to 30 days. Barbiturates are excreted in the urine in unchanged forms, hydroxylated derivatives, carboxylated derivatives and glucuronide conjugates.
Buprenorphine (BUP)
Buprenorphine is a derivative of thebaine, is an opioid that has been marketed in the United States as the Schedule V parenteral analgesic Buprenex. In 2003, based on a reevaluation of available evidence regarding the potential for abuse, addiction, and side effect, DEA reclassified buprenorphine from a Schedule V to a Schedule III narcotic. Buprenorphine resembles morphine structurally but has a longer duration of action than morphine and can be administrated sublingually as an analgesic. In October 2002, FDA approved the use of a buprenorphine monotherapy product, Subutex, and a buprenorphine/naloxone combination product, Suboxone, for the treatment of opioid addiction. Subutex and Suboxone are the first narcotic drugs available under the US Drug Act (DATA) of 2003 for the treatment of opiate dependence that can be prescribed in the US in a physician’s workplace. It has also been shown that buprenorphine has abuse potential and may itself cause dependency. In addition, several deaths have been recorded as a result of overdose with intravenously injected buprenorphine in conjunction with other psychotropic drugs such as benzodiazepines. Buprenorphine is metabolized primarily by n-dealkylation to form glucuronide-buprenorphine and glucuronide-norbuprenorphine.
Cocaine (COC)
Cocaine Derived from the leaves of coca plant, cocaine is a potent central nervous system stimulant as well as a local anesthetic. Some of the psychological effects induced by cocaine are euphoria, confidence and a sense of increased energy, accompanied by increased heart rate, dilation of the pupils, fever, tremors and sweating. Continued ingestion of cocaine could induce tolerances and physiological dependency which leads to its abuse. Cocaine is used by smoking, intravenous, intranasal or oral administration and excreted in the urine primarily as benzoylecgonine in a short period. Benzoylecgonine has a biological half-life of 5 – 8 hours, which is much longer than that of cocaine (0.5 – 1.5 hours) and can be generally detected for 12 – 72 hours after cocaine use or exposure.
EDDP
EDDP 2-Ethylidine-1,5-dimethyl-3,3-diphenylpyrrolidine, is the primary metabolite of methadone. Methadone is a controlled substance and is used for detoxification and maintenance of opiate dependent patients. Patients on methadone maintenance may exhibit methadone (parent) levels that account for 5-50% of the dosage and 3-25% of EDDP in urinary excretion during the first 24 hours. The detection of EDDP is more beneficial than traditional methadone screening, in that EDDP exists only in urine from individuals that ingested methadone. The tampering of specimens by spiking the urine with methadone can be prevented. Secondly, renal clearance of EDDP is not affected by urinary pH, therefore the EDDP test provides a more accurate result of methadone ingestion than the methadone parent screen.
Methadone (MTD)
Methadone is a synthetic opioid, clinically available. It is used clinically for the treatment of severe pain and in maintenance programs for morphine and heroin addicts. Methadone acts on the central nervous and cardiovascular systems to produce respiratory and circulatory depression. Methadone also produces miosis and increases the tone of smooth muscle in the lower gastrointestinal tract while decreasing the amplitude of contractions. Acute higher doses induce analgesia, sedation, respiratory depression and coma. After methadone administration, the major urinary excretion products are methadone and its metabolites, EDDP and EMDP. Large individual variations in the urine excretion of methadone are output of methadone from 5-22%. Typically, following a 5 mg oral dose, methadone and EDDP account for 5% of the dose in the 24-hour urine. In those individuals on maintenance therapy, methadone may account for 5 to 50% of the dose in the 24-hour urine and EDDP may account for 3 to 25% of the dose.
Methamphetamine (M-AMP)
Methamphetamine is the most popular synthetic derivative of the amphetamines. It is a potent sympathomimetic agent with therapeutic applications. Acute large doses lead to enhanced stimulation of the central nervous system and induce euphoria, alertness, reduced appetite, and a sense of increased energy and power. More acute response produces anxiety, paranoia, psychotic behavior, and cardiac dysrhythmias. Methamphetamine is excreted in the urine as amphetamine and oxidized and deaminated derivatives. However, 10-40% of methamphetamine is excreted unchanged. Methamphetamine is generally detectable in the urine for 3 to 5 days after use.
MDMA
MDMA Methylenedioxymethamphetamine (Ecstasy) is a designer drug first synthesized in 1914 by a German drug company for the treatment of obesity. Those who take the drug frequently report adverse effects, such as increased muscle tension and sweating. MDMA is not clearly a stimulant, although it has, in common with amphetamine drugs, a capacity to increase blood pressure and heart rate. MDMA does produce some perceptual changes in the form of increased sensitivity to light, difficulty in focusing, and blurred vision in some users. Its mechanism of action is thought to be via release of the neurotransmitter serotonin. MDMA may also release dopamine, although the general opinion is that this is a secondary effect of the drug. The most pervasive effect of MDMA, occurring in almost all people who have taken a reasonable dose of the drug, is to produce a clenching of the jaws. The MDMA Ecstasy Test Strip yields a positive result when Methylenedioxymethamphetamine in urine exceeds 500 ng/mL.
Ketamine (KET)
Ketamine is a derivative of phencyclidine. It is used medically as a veterinary and human anesthetic. Certain doses of ketamine can cause dream-like states and hallucinations. In high does, ketamine can cause delirium, amnesia, impaired motor function, high blood pressure, depression, and potentially fatal respiratory problems. Ketamine is metabolized in the liver and excreted through the kidney. The half-life of ketamine in the body is around three hours.
Opiates (OPI)
Opiate Opioid analgesics are comprised of a large group of substances that control pain by depressing the central nervous system. Acute high dose used by abusers or addicts can cause depressed coordination, disrupted decision, decreased respiration, hypothermia and coma. Morphine is excreted unmetabolized and is the marker metabolic product of opiates. Morphine and morphine glucuronide are detectable in urine for several days after opiates dose.
Oxycodone (OXY)
Oxycodone is known as Oxycontin, Roxicodone and is an ingredient of Percodan, Percocet, Roxicet and Tylox. Oxycodone is a semi-synthetic opiate derived from opium. Like other opiates, oxycodone is characterized by its analgesic properties, and the tendency for users to form a physical dependency and develop tolerance with extended use. Oxycodone is usually administered in combination with non-opiate analgesics such as acetaminophen and salicylates for the relief of moderate to severe pain. Oxycodone is a central nervous system depressant that may cause drowsiness, dizziness, lethargy, weakness and confusion. Toxicity in an overdose of oxycodone can lead to stupor, coma, muscle flaccidity, severe respiratory depression, hypotension, and stripiac arrest. Oxycodone is metabolized by N- and O-demethylation. One of the metabolites, oxymorphone, is a potent narcotic analgesic, while the other, noroxycodone, is relatively inactive. Between 33 to 61% of a single dose of oxycodone is excreted in a 24-hour urine collection and consists of 13-19% free oxycodone, 7-29% glucuronide conjugated oxycodone, 13-14% glucuronide conjugated oxymorphone and an unknown amount of noroxycodone. The detection time window of oxycodone is 1-3 days following use.
Phencyclidine (PCP)
Phencyclidine commonly known as PCP, is a hallucinogen which interacts with dopamine, cholinergic and adrenergic systems. It has dose dependent stimulant, depressant, hallucinogenic and psychological effects. PCP is mostly administered by oral or intravenously. Even moderate amounts of PCP, from 5 to 100 ng/mL, can result in psychotic, violent and self-destructive behaviors. At high doses, from 100 to 500 ng/mL, PCP can cause convulsions, hypertension, prolonged coma, absent peripheral sensation, and even death. PCP is metabolized via hydroxylation, oxidation, and conjugation with glucuronic acid in the liver. About 10% of the does is excreted in urine as unchanged drug. For chronic users, PCP can be detected in the urine for 7 to 8 days after drug administration.

Propoxyphene (PPX)
Propoxyphene is a prescription drug for the relief of pain. Although slightly less selective than morphine, Propoxyphene binds primarily to opioid receptors and produces analgesia and other CNS effects that are similar to those seen with morphine-like opioids. It is likely that at equianalgesic doses the incidence of side effects such as nausea, anorexia, constipation, abdominal pain, and drowsiness are similar to those of codeine. After oral administration, concentrations of Propoxyphene in plasma reach their highest values at 1 to 2 hours. There is great variability between subjects in the rate of clearance and the plasma concentrations that are achieved. The percentage of excreted unchanged Propoxyphene in urine is less than 1%. In humans, the major route of metabolism is N-demethylation to yield norpropoxyphene. Norpropoxyphene has a longer half-life (30 to 36 hours) than parent Propoxyphene (6 to 12 hours), and its accumulation with repeated doses may be responsible for some of the observed toxicity.

Marijuana (THC)
THC The agents of Marijuana that cause various biological effects in humans are called cannabinoid. Cannabinoid is a central nervous stimulant that alters mood and sensory perceptions, produces loss of coordination, impairs short term memory, and produces symptoms of anxiety, paranoia, depression, confusion, hallucination, and increased heart rate. Large doses of cannabinoid could cause the development of tolerances and physiological dependency and lead to abuse. A tolerance to the cardiac and psychotropic effects can occur and withdrawal syndrome produces restlessness, insomnia, anorexia and nausea. Δ 9-THC is the primary active ingredient in cannabinoids. The main metabolite excreted in the urine is 11-nor- Δ 9-THC-9-COOH, which are found within hours of exposure and remain detectable in the urine for 3-10 days after smoking.
Tramadol (TML)
Tramadol is a quasi-narcotic analgesic used in the treatment of moderate to severe pain. It is a synthetic analog of codeine but has a low binding affinity to the mu-opioid receptors. Large doses of tramadol can develop tolerance and physiological dependency and lead to its abuse. Tramadol is extensively metabolized after oral administration. Approximately 30% of the dose is excreted in the urine as unchanged drug, whereas 60% is excreted as metabolites. The major pathways appear to be N- and O- demethylation, glucuronidation or sulfation in the liver.
Tricyclic antidepressants (TCA)
TCA Tricyclic antidepressants, commonly known as TCAs, are a group of antidepressant drugs. TCAs are mostly administered by oral or intramuscularly. The progressive symptomatology of TCAs includes agitation, confusion, hallucinations, hypertonicity, seizures and EKG changes. Nortriptyline, Desipramine (Pertofran) and Imipramine (Tofranil) are the most often used TCAs. TCAs half-life varies from a few hours to a few days. TCAs are excreted with less than 1% of the unchanged drug.
Methylphenidate (MPD)
Methylphenidate is most known by the Novartis trademark name Ritalin, which is an instant-release racemic mixture. There are also a variety of formulations and generic brand names exist. Methylphenidate is a psychostimulant drug for the treatment of attention-deficit hyperactivity disorder, Postural Orthostatic Tachycardia Syndrome, and narcolepsy. It may also be prescribed for off-label use in treatment-resistant cases of lethargy, depression, neutral insult, obesity, and rarely other psychiatric disorders such as obsessive-compulsive disorder. Methylphenidate, like other stimulants, increases dopamine levels. The abuse potential is increased when methylphenidate is crushed and snorted or when it is injected producing effects almost identical to cocaine. Cocaine-like effects can also occur with very large doses taken orally. Methylphenidate has a high potential for drug dependence and additive abuse due to its similar pharmacologically to cocaine and amphetamines. Internationally, methylphenidate is a Schedule II drug under the Convention on Psychotropic Substances. In the United States, methylphenidate is classified as a Schedule II controlled substance, which is the designation used for substances that have a recognized medical value but present a high likelihood for abuse because of their addictive potential.
Fentanyl (FTL)
Fentanyl is a synthetic opioid. It has the brand names of Sublimaze, Actiq, Duragesic, Fentora and others. Fentanyl is approximately 100 times more potent than morphine, with 100 micrograms of fentanyl approximately equivalent to 10 mg of morphine or 75 mg of meperidine in analgesic activity. Fentanyl is a potent narcotic analgesic with rapid onset and short duration of action. Historically, it has been used to treat chronic breakthrough pain and is commonly used pre-procedures. Illicit use of pharmaceutical fentanyls first appeared in the mid-1970s. Because the effects of fentanyl last for only a very short time, it is even more addictive than heroin. The regular users may become addicted very quickly. Fentanyl is much more potent than heroin, and tends to produce significantly worse respiratory depression, making it somewhat more dangerous than heroin to users. The overdose of fentanyl has caused death. In the United States, fentanyl is classified as a Schedule II controlled substance.
Synthetic cannabic (SPICE/K2)
K2 Synthetic cannabis is a psychoactive herbal and chemical product that, when consumed, mimics the effects of cannabis. It is best known by the brand name K2 and Spice, both of which have largely become genericized trademarks used to refer to any synthetic cannabis product. The studies suggest that synthetic cannabinoid intoxication is associated with acute psychosis, worsening of previously stable psychotic disorders, and also may have the ability to trigger a chronic (long-term) psychotic disorder among vulnerable individuals such as those with a family history of mental illness. A large and complex variety of synthetic cannabinoids, most often cannabicyclohexanol, JWH-018, JWH-073, or HU-210, are used. As of March 1, 2011, five cannabinoids, JWH-018, JWH-073, CP-47, JWH-200 and cannabicyclohexanol are illegal in US because these substances have the potential to be extremely harmful and, therefore, pose an imminent hazard to the public safety.
Clonazepam (7-ACL)
Clonazepam is a chlorinated derivative of nitrazepam having anticonvulsant, muscle relaxant, and very potent anxiolytic properties. It is marketed as the prescription drug under the names of Klonopin, Ravotril, Rivotril or Rivatril. Clonazepam has an unusually long half-life of 18-50 hours in human body, making it generally considered to be among long-acting benzodiazepines. Clonazepam has a fast onset of action and high effectiveness rate and low toxicity in overdose but has drawbacks due to adverse reactions including paradoxical effects, drowsiness, and cognitive impairment. Cognitive impairment can persist for at least 6 months after withdrawal of clonazepam. Clonazepam is largely bound to plasma proteins. Clonazepam is rapidly and completely absorbed after oral administration. Maximum plasma concentration of Clonazepam is reached within 1 to 4 hours after oral administration. Clonazepam is highly metabolized with less than 2% unchanged in urine. The metabolites include 7-aminoclonazepam (7-ACL), 7-acetaminoclonazepam and 3-hydroxy clonazepam.
Cotinine (COT)
Cotinine is an alkaloid found in tobacco and is also a major metabolite of nicotine. Cotinine is used as a biomarker for exposure to tobacco smoke and has also been sold as an anti-depressant under the brand name of Scotine. Cotinine has an in vivo half-life of approximately 20 hours and is typically detectable for several days after the use of tobacco. The level of cotinine is proportionate to the amount of exposure to tobacco smoke. In urine, values between 11 ng/mL and 30 ng/mL may be associated with light smoking or passive exposure. The cotinine levels in active smokers typically reach 500 ng/mL or more.
Alcohol
Alcohol: Acute alcohol intoxication can lead to loss of alertness, coma, and even death. Long term effects include internal organ damage and birth defects. The blood alcohol concentration (BAC) at which a person becomes impaired is variable. The United States Department of Transportation (DOT) has established a BAC of 0.02% (0.02 g/dL) as the cut-off level at which an individual is considered positive for the presence of alcohol. Since urine alcohol concentration is normally higher than that in saliva and blood, the cut-off concentration for alcohol in urine is set at 0.04%.
This test is based on the high specificity of alcohol oxidase (ALOx) for ethyl alcohol in the presence of peroxidase and enzyme substrate such as tetramethylbenzidine (TMB) as shown in the following:
![]()
The distinct color on the reactive pad could be observed in less than 20 seconds after the urine samples migrates over the reaction pad with the ethyl alcohol concentration greater than 0.04%. It should be pointed out that other alcohols such as methyl, propanyl and allyl alcohol would develop the similar color on the reactive pad. However, these alcohols are not normally present in urine.
More Parameters
We have a variety of additional parameters available beyond those listed below. If you have any questions or would like more information, feel free to contact us.
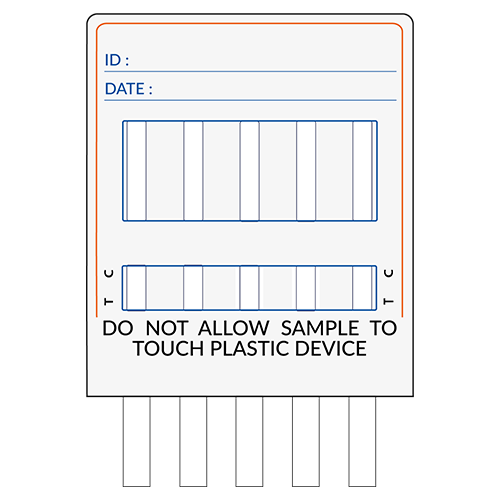
Adulteration Tests
MP Adulteration tests are built-in firm plastic strips to which options of 1 up to 6 different reagent areas can be affixed. Adulteration tests are ready-to-use and disposable. No equipment is required for its use. Only fresh and uncentrifuged urine samples without preservatives are to be used.
It provides tests for :
Test results may be useful for assessing the integrity of the urine sample while running drugs-of-abuse & alcohol testing, for example, whether the sample is possibly diluted with water or other liquids as indicated by the creatinine and specific gravity tests. Adulteration test detects whether the sample contains commercially available adulterants including nitrite, glutaraldehyde, and other oxidizing agents.
It can also assess whether the sample is possibly contaminated by acidic (vinegar) or basic (ammonia solution) adulterants as indicated by the pH test.